The Christopher & Dana Reeve Foundation Paralysis Resource Center (PRC) will host a FREE webinar on traveling by road or on a train for individuals living with paralysis. The webinar will be held on Wednesday, October 30, 2019.
The Americans with Disabilities Act guarantees that travelers with disabilities receive equal treatment under the law. While this is true, wheelchair users have to consider their travel options carefully before making the trip depending on their situation. Traveling by plane may be the quickest source of transportation, but it’s not always the most efficient way to travel when considering all factors as a wheelchair user. This presentation will stress the importance and available options for traveling by car or train, as there are aspects people living with paralysis should consider before taking a trip. This includes the advantages and disadvantages of both modes of travel, and amenities travelers are entitled too as they embark to their desired destination.
“There are several individuals in our community who are not able to travel by plane due to cost or health conditions,” said Angela Cantillon, Director of Operations for the Paralysis Resource Center. “With this webinar, the audience can gain access to tools for accessible, cost-efficient ways of traveling to see their families and help combat the feeling of isolation.”
The webinar will be hosted by John Morris, a field expert and an advocate for accessible travel. Included in the webinar will be topics such as destinations available through railways and roadways, Road Trips with a Vehicle, Intercity Bus Services, and Train Travel in the USA.
The hour-long webinar will be held on at 2:00pm EST. Registry for the webinar can be found on the Reeve Foundation’s events page.
What’s your preferred mode of travel transportation? Share with us!
A diagnosis of a chronic condition such as Crohn’s disease, ulcerative colitis, cancer or diabetes can bring a swirl of thoughts and emotions. There may be relief at finding an explanation for bothersome symptoms, but that relief is often quickly overshadowed by insurance issues, financial concerns and worry about the future.
If you’ve recently received a chronic diagnosis, take it one step at a time to navigate the road ahead. Here are some tips:
Understand Your Condition
Arming yourself with information is critical when you receive a life-altering diagnosis. It’s important to understand everything you can about the condition, including known causes, symptoms you may experience, what you can expect as the disease progresses and more.
Identify Treatment Options
A big part of your research will likely involve your treatment options. If your doctor has outlined multiple options for treatment, you’ll want to investigate each one thoroughly so you can understand the benefits and risks, as well as deciding which option is the best fit for your particular circumstances. You’ll also want to confirm that your treatment is covered by your health insurance and at what level.
Handle Insurance Issues
Most people assume that if they have health coverage, they can count on at least a portion of the treatments and medications their doctor recommends being covered. In many cases, that’s true, although the exact coverages depend on variables like your plan, deductible and more.
However, there are also some circumstances in which you may experience a delay before you’re able to follow your doctor’s treatment orders. One example is step therapy – a protocol sometimes used by health insurance companies that requires patients to try and fail on one or more lower cost medications before they will provide coverage for the medication originally prescribed by the patient’s provider.
photo credit: CDC
Step therapy is also known as “fail first” because it requires a patient to fail on an insurer-preferred drug first. Unfortunately, for patients with inflammatory bowel diseases (IBD), like Crohn’s disease and ulcerative colitis, this protocol may result in worsened health outcomes. A survey by the Crohn’s & Colitis Foundation found that as many as 40 percent of IBD patients had been subject to step therapy, and 58 percent of those patients were required to fail two or more drugs before being granted access to the drug their doctor originally prescribed.
“During these delays in optimal treatment, patients are at risk, not only for their physical well-being, but also for their quality of life,” said Dr. Ross Maltz, co-chair of the Government and Industry Affairs Committee of the Crohn’s & Colitis Foundation’s National Scientific Advisory Committee.
“In some instances, insurance policies can impede patient access to the care they need and affect the patient and provider decision-making process.”
Groups are working to change this process through legislative reform but, in the meantime, if you are subject to a step therapy requirement by your insurance provider, you can appeal. The best approach is to work with your doctor to prepare a written letter that contains:
· A clear statement that you are appealing a denial of coverage for your prescribed medication
· The name of the medication that was denied
· A detailed explanation of previous treatments or factors that led your doctor to prescribe the denied medication
· Any studies or evidence that support the use of the prescribed medication
· The specific health risks you experience now or may in the future without the medication that was originally prescribed
· A clearly stated request for approval of the specific prescription, including the medication name and dosage
Becoming a dog trainer (or service dog trainer) can be very rewarding, but it is also a lot of work. Having a love of animals is just the beginning — the most experienced dog trainers understand that often the most difficult part of the gig is working with people!
You may be surprised to learn that there are no legally-mandated standards or certifications for service dog trainers — or pet dog trainers. Anyone can decide to train dogs and start their own business or training organization. Most trainers are self-taught or have learned techniques through other trainers, books, online courses, videos or short seminars. Some of the best trainers do not have formal training themselves. That being said, if you are interested in becoming a trainer we highly suggest some kind of formal training.
There are a few dozen schools around the country that train service dog trainers. Most are small and began with experienced dog trainers (some began with training military working dogs, police dogs or other working dogs) who moved into training service dogs for disabled individuals and then decided to help train trainers too. One of the best places to learn how to become a service dog trainer in the country (and possibly the world) is Bergin University. If you’re really looking for the finest service dog training education possible, Bergin is the hands-down go-to school.
The ADA is written to allow disabled individuals to use their service dogs in public with as few barriers as possible. If access were not as open, every building, restaurant and dry cleaner in the country could stop disabled individuals with their service dogs and demand proof of training. The ADA specifically states that if someone says their dog is a service dog they are to be taken at their word, regardless if it has been certified by a state or other authority. See below:
The ADA states in section § 35.136 service animals part (f): “A public entity shall not require documentation, such as proof that the animal has been certified, trained, or licensed as a service animal.” You can view the full ADA law here: https://www.ada.gov/regs2010/titleII_2010/titleII_2010_withbold.htm
The ADA is also designed so that disabled individuals may train their own service dogs. Program-trained service dogs can be very expensive and out of budget for many disabled individuals. Some service dogs may cost upwards of $10,000.
About USSDR
With the input from over 100 service dog handlers in America, the United States Service Dog Registry (USSDR) represents the most democratic realization of an assistance animal registry and training and behavior standards agreement to-date. The results are a registry with completely free and voluntary online self-registration hosted by an independent, non-governmental, privacy-conscious and secure service.
USSDR is designed with input from experienced trainers and service dog owners who believe there should be an opportunity for those who wish to voluntarily and knowingly comply with not only the ADA law, but also an additional and specific set of community-defined training and behavior standards. These training and behavior standards go above and beyond the ADA and the basic foundations of a Public Access Test.
A Higher Standard for Service Dogs and their Handlers
USSDR’s purpose is to allow someone the opportunity to voluntarily hold themselves and their animal accountable to a higher standard by publicly signing a specific set of training and behavior standards that goes above and beyond the law. Simply registering with with USSDR or any state does not qualify an animal or an individual as a service dog Ttam or provide any special rights, legal or otherwise. If someone is found not to comply with USSDR’s training or behavior standards their registration can be removed or suspended.
What does Registration with USSDR mean?
USSDR is an extra step that goes above and beyond the law. Under the law it is not required that service and assistance dog teams show or have identification in the form of a vest, special harness, training certificate or registration. Nor is it required that animals are officially trained, certified or registered with any state, federal or independent organization.
USSDR hopes to help reduce the number of people abusing the ADA by requiring registrants to understand that intentionally misrepresenting an animal as service or assistance animal for any reason is not only unethical, it is also illegal. All registrants are required to understand and accept the following:
What is involved with training and using a service or assistance animal
How important their behavior, and that of their service or assistance dog, is to the general public and other service and assistance animal teams
The definition of a service or assistance animal
The minimum training standards for a service or assistance animal
What is involved with a Public Access Test
Originally published by AnythingPawsable; reprinted with permission.
Epilepsy is brain disorder that causes repeated seizures. About 3 million U.S. adults aged 18 years or older have active epilepsy. Nearly 1 million of those adults are aged 55 or older. As our population ages, there will be even more older people with epilepsy in the coming years.
Epilepsy is more likely to develop in older adults because some risk factors for epilepsy are more common in older adults, such as:
Diseases that affect brain function (such as Alzheimer’s disease)
Brain tumors
About half of older adults who are told they have epilepsy do not know the cause.
Epilepsy can affect people at any age, but it’s more likely to develop in older adults.
photo credit: AARP
How Do I Know If It’s Epilepsy?
It isn’t always easy to tell when you or someone you care for develops epilepsy later in life. That’s because seizures may be hard to recognize in older adults and may go unnoticed. For example, memory problems, confusion, falls, dizziness or sensory changes (like numbness) are often blamed on “getting older.” However, these can actually be signs of seizures.
There are many different signs of seizures because there are many types of seizures. In the movies and on TV, a person is often shown falling to the ground, shaking and becoming unaware of what’s going on around them. That’s one kind of seizure, but it’s not the most common. More often, a person having a seizure may:
Seem confused
Stare into space
Wander
Make unusual movements
Can’t answer questions or talk
When these signs occur more than once and often in the same pattern, they could be signs of seizures.
If an older adult is showing these signs, it is important for them to talk to a health care provider. Most adults with epilepsy have good seizure control with medicines. Epilepsy specialists can help older adults find the right treatment. Find an epilepsy specialist near you through the Epilepsy Foundation.
How Is Epilepsy Challenging for Older Adults?
Adults who develop epilepsy later in life may have a hard time managing the disorder. Eight in 10 adults aged 65 or older have more than one chronic health condition. It can be hard to balance epilepsy treatment when taking medicines for other health problems. Many epilepsy medicines also have side effects such as bone loss or dizziness, which can make someone more likely to fall and become injured.
Epilepsy can also affect a person’s daily life if seizures limit their ability to drive or if they live alone. After a lifetime of being independent, losing the ability to drive or take care of themselves can be especially hard for older adults.
Caregivers should learn how to recognize seizures in older adults.
How Can You Help?
Seizure first aid is easy to give and involves keeping the person safe until the seizure stops on its own and knowing when to call 911 for emergency help.
If you work at an adult day care center, senior center, long-term care facility, nursing home, in home health care or another senior-serving organization, there is special training available. Seniors & Seizures is a free online or in-person course offered by the Epilepsy Foundation. You can get free continuing education credits for participating.
Do I Call 911?
Seizures do not usually require emergency medical attention. Only call 911 if one or more of these are true:
The person has never had a seizure before.
The person has difficulty breathing or waking after the seizure.
The seizure lasts longer than 5 minutes.
The person has another seizure soon after the first one.
The person is hurt during the seizure.
The seizure happens in water.
The person has a health condition like diabetes, heart disease or is pregnant.
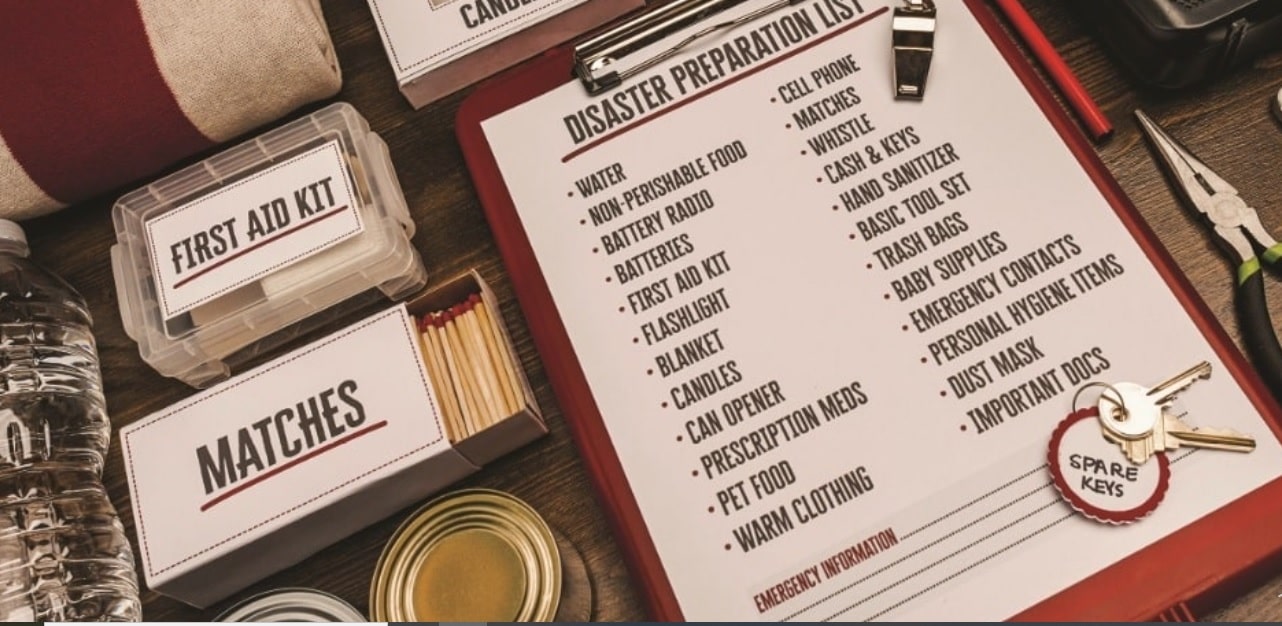
Recently, at the start of the 2019 hurricane season, the National Council on Disability (NCD)—an independent federal agency—released its latest report, titled, Preserving Our Freedom: Ending Institutionalization of People with Disabilities During and After Disasters.
NCD, which advises the President and Congress, examined available data from several major storms and disasters and found that people with disabilities are frequently institutionalized during and after disasters due to conflicting federal guidance; a lack of equal access to emergency and disaster-related programs and services; and a lack of compliance with federal law.
Over 47 million people were impacted by Hurricanes Harvey, Irma and Maria, and based on disability prevalence statistics, as many as nearly 12 million of them may have been people with disabilities.
The report, which focused on the reasons people with disabilities experience involuntary institutionalization as a result of disasters, found that the Federal Government offers conflicting guidance on the topic. For example, Department of Justice (DOJ) guidance states that “people should receive services in the most integrated setting appropriate to the needs of the person, and only persons who require the type and level of medical care that would ordinarily be provided by trained medical personnel in a nursing home or hospital” should be placed in those more restrictive settings. In contrast, the Department of Health and Human Services (HHS) Centers for Medicare and Medicaid Services (CMS) repeatedly issues waivers to their institutional placement rules during disasters, allowing states to place disaster-impacted people with disabilities in nursing homes and other institutional settings.
The report also found that recipients of federal funds do not have training for how to comply with federal requirements to provide equal access to emergency and disaster-related programs and services when using federal dollars, nor do they have the cultural competence to interact with people with disabilities and often adhere to stereotypes and myths about disability that results in institutional placement. As a result of unnecessary institutionalizations of people with disabilities during and after disasters, people with disabilities often go unaccounted for, families are separated from loved ones, working individuals with disabilities often become unemployed, and students with disabilities are often excluded from returning to school with their peers.
NCD’s recommendations to policymakers include the following:
Congress should require CMS to establish a process for Medicaid portability among states and territories during disasters to ensure uninterrupted health maintenance and medical care in the least restrictive environment for Medicaid recipients.
Congress should appropriate funds for FEMA, HHS, and HUD to fund Independent Living Center staff and other affordable and accessible housing experts to provide individual and household disaster case management focused on the transition and permanent housing needs of disaster-impacted people with disabilities.
Congress should require that HHS establish a data collection system and that data collection begins immediately after the next federally declared disaster. The system must identify impacted individuals moved to an institutional setting and quantify movement and displacement of all impacted people in the aggregate.
The U.S. Department of Education (ED) should issue a policy directive to require school systems to include an individualized emergency plan for uninterrupted delivery in every student’s IEP or 504 plan to comply with the Free and Appropriate Public Education requirement in IDEA and in the Rehabilitation Act.
People with disabilities have a right to equal access to emergency services. Registries have both impeded equal access solutions and established inadequate alternatives for using federal funds. NCD recommends that no federal funds, including but not limited to federal funds from the U.S. Department of Homeland Security (DHS) and HHS, be used in development, deployment, and maintenance of emergency ‘special needs’ registries intended to include people with disabilities.
Read the full report at https://ncd.gov/publications/2019/preserving-our-freedom.
Losing my best friend was one of the best things that ever happened to me…
Almost five years ago, I lost my dear friend Jessica as a result of her lifelong battle with muscular dystrophy (MD), a genetic condition that results in weakening and deterioration of muscles in the body.
Jessica spent her whole life in a wheelchair, watching others experience things she thought she could never. Fortunately, she was born into the most amazing family ever! They never ever let disability impact her experiences in life (or her brother’s, who also has MD). They took several family vacations, included her in community events, had wild and crazy parties at their house and even had the courage to send her off to Central Michigan University where she nearly completed her master’s degree.
As a result of Jessica’s muscular dystrophy, she required assistance for many of her daily needs: dressing, using the restroom, taking a bath, picking things up off the ground, brushing her hair and other daily activities so many of us take for granted. Her ability to navigate life, advocate for herself and show so much compassion for others (never feeling sorry for herself) was admirable and incredible to say the least.
Jessica and I lived together at Central Michigan University; and although I have many stories of our fun times, I will keep those to myself for now! This was probably the first time I truly understood how challenging accessibility can be. It was our goal to not hold back due to her disability, but the reality is that some bathrooms were impossible to get into, house parties were very challenging (but luckily plenty of strong, drunk fellas were there to help lift her chair) and trying something new was always a risk because it may be an hour before the taxi with a lift would be able to come back to pick us up.
photo courtesy of Meegan Winters
Seeing The Next Impactful Chapter
During the last few months of Jessica’s life is when I learned the most. She was suffering, she was unhappy, she wasn’t even able to eat solid foods anymore (one of her favorite things to do… haha). I selfishly didn’t want to let her go though. How would I survive not talking to her every day? Jessica assured me that she would be with me even after she passed and she would be happier than ever. I believe both of these statements now. She IS with me on the journey creating Able Eyes, a website I launched that is designed to help people with both physical and invisible disabilities access the community with ease and comfort. This is what she would have wanted to do and I believe this journey is in honor of her and also a part of her.
Quite simply, it is because of her passing that this amazing digital service was developed, and Jessica and I are both able to follow our true paths and passion for helping others. In addition to my experience with Jessica, I’ve also worked with children and adults on the autism spectrum for over 15 years as a teacher and administrator, which has enhanced by drive to help others.
What is Able Eyes?
Here’s a Q&A with everything you need to know about Able Eyes.
1. What is Able Eyes?
Able Eyes (www.AbleEyes.org) is diligently working to create inclusive communities on a national scale through the use of 360 virtual tours of public spaces. Able Eyes does not rank or judge accessibility of locations. You are able to put in your zip code to view the businesses in your area that have virtual tours to allow patients to become more comfortable with the space before physically visiting.
Able Eyes believes in helping ALL members of your community (and communities across the US) access local businesses without stress. We help people “Know Before You Go” by creating or adding virtual tours to our website for people of all abilities but specifically for those with physical and invisible disabilities.
For businesses, Able Eyes virtual tours offer a creative option to help the community while gaining a powerful marketing tool for website and social media use.
Meegan Winters shows an Able Eyes business. | photo courtesy of Able Eyes
2. Why Able Eyes?
26% of the population now has a disability (1-in-4). Of that 26%, 80% are invisible (autism, anxiety, PTSD, ADHD, etc). Currently, we do not have any accommodations in place to help those with invisible disabilities access the community. Able Eyes helps both, as well as those without disabilities that like to use virtual tours.
As a special educator and administrator working with students on the autism spectrum, I identified a need and the importance of a tool such as Able Eyes several years before I actually took action. So many families are NOT going out into the community if they have a child or family member with special needs. This could be the unknown accessibility for a wheelchair user, the lack of predictability for a child on the spectrum or any number of challenges one might face with different needs. In all scenarios, both the family and the individual are sacrificing their quality of life, their potential and their experiences because of the unknown. Able Eyes is the window to the future that will help change all of this. One story will always stand out to me: when I was a teacher in the classroom, I had a parent call one morning in tears. Of course, I immediately assumed something was wrong or she was upset. But, in fact, they were happy tears! She went on to tell me the very detailed story of her family’s VERY FIRST trip out to a restaurant as a family of four (her son was 10-years-old). Could you imagine 10 years passing and never having an opportunity to experience a meal out as a family?
3. Who is Able Eyes for?
The primary users are parents, teachers, therapists and individuals of various abilities. In addition to to the virtual tours, Able Eyes also has a Video Modeling library; short “how to” or “what to expect videos” to either teach expectations or prepare a person for an upcoming activity. The primary goal is to ensure all people are comfortable, have access and have the tools to live their best life.
The Able Eyes Mission
Do you know someone with autism? If you do, you know that visiting new locations can cause a LOT of anxiety and sometimes results in loud, disrupting and even destructive behaviors.
Do you know a person that uses a wheelchair? If you do, you know that going out into the community can be a challenge because of curbs, parking, small restrooms, steps, etc.
Do you know someone that has experienced trauma or has anxiety? If you do, you know that something that seems simple to many can feel like drowning, such as large crowds, tight spaces or anything out of the ordinary.
Do you know anyone with or without a disability that experiences challenges out in the community?
Do YOU often Google places to learn more, read a menu or take a tour before you visit?
The mission of Able Eyes is to provide visual, state of the art experiences/teaching tools to children and adults with disabilities. Able Eyes provides a user friendly platform to teach skills, and explore environments from several different perspectives. Our ultimate goal is to make businesses and public venues more accessible for people of all abilities by offering visual tours, making them “Able Eyes Accessible.”
In the past two decades, an overriding concern for educators, public health experts and policymakers has been the steadily rising number of children with special needs. According to estimates by the Centers for Disease Control and Prevention (CDC), one in seven children is affected by some form of disability, which places a severe strain on public resources and takes a heavy toll on families — both from an emotional and financial perspective.
In recent years, some of the attention has shifted to alternative solutions, and equine-assisted therapy (EAT) is proving to be especially effective for children with special needs, explains Alexa Rostovksy, a student at the Harvard-Westlake School in Los Angeles, California. She has witnessed the benefits first-hand through her involvement with Ahead With Horses, a nonprofit organization helping children with disabilities maximize their potential through developmental therapy, education and recreation.
photo credit: Ahead With Horses
In EAT, individuals interact with horses and therapeutic riding instructors to acquire communication, socialization, motor control and sensory processing skills. Through a series of exercises, children with severe disabilities apply traditionally practiced methods while engaging with the animals and performing tasks in motion on horseback. This provides a multi-dimensional challenge in an environment outside of their familiar one. “It is incredible to witness a little boy go from barely standing up by himself to being on top of a moving horse with a wide smile on his face. I have met many parents who tell me the therapy has transformed their child’s life,” says Alexa Rostovsky who works with kids who have disabilities or behavioral issues or come from troubled backgrounds. With support from volunteers like her, they meet and bond with their assigned horse, climbing atop it and learning to ride. The activity has been shown to build core strength as well as help children gain self-esteem, discipline and empathy while also experiencing joy.
EAT is often used in treating a wide spectrum of conditions, among them substance abuse, behavioral disorders, learning difficulties, ADD/ADHD, autism, Asperger’s, grief, loss, trauma, bipolar disorders and depression. “Horses have no preconceived expectations or motives, and they are non-judgmental, highly intelligent and exceedingly perceptive, so they connect with people in a completely new way,” Alexa Rostovsky points out, adding, “This is different from anything these children have experienced at school. It is not about discipline or grading but about facing something entirely foreign and reaching their own milestones. Witnessing the confidence and pride that comes with accomplishing something so new to them is exceptionally rewarding.”
As recommended by the National Council on Disability (NCD), all U.S. dental schools must now revamp their curricula and training programs to be inclusive of patients with intellectual and developmental disabilities (ID/DD).
The Council on Dental Accreditation (CODA) recently passed votes requiring dental schools to now train their students in managing treatment of patients with ID/DD. Previously, patients with ID/DD were largely unable to obtain dental care treatment because dental students were simply not required to learn to manage their treatment.
“Every dental patient in America deserves the same care, whether or not they have a disability,” said NCD Chairman Neil Romano. “NCD applauds this decision that we view as necessary for people with ID/DD to obtain critical access to dental treatment, which is critical to the total health of all people.”
CODA held and passed four related votes regarding the predoctoral dental, orthodontics, dental hygiene, and dental assistant programs:
For predoctoral programs and orthodontics programs, dental students must be trained to assess and manage the treatment of patients with “special needs.”
For dental hygiene programs, students must be competent in providing care to “special needs” patient populations.
For dental assistant programs, students must be familiarized with patients with “special needs” including patients whose medical, physical, psychological, or social conditions make it necessary to modify normal dental routines.
CODA generally defines people with “special needs” as people with developmental disabilities, cognitive impairment, complex medical problems, significant physical limitations, and the vulnerable elderly.
Changes for the predoctoral dental, dental hygiene, and dental assistant programs are required to take effect by July 1, 2020, with changes to the orthodontics programs required by Jan. 1.
photo credit: American Dental Association
NCD first made recommendations to CODA following its 2017 issue brief “Neglected for Too Long: Dental Care for Patients with Intellectual and Developmental Disabilities,” in which NCD’s findings included:
Adults with developmental disabilities are at risk for multiple health problems including poor oral health.
People with I/DD regularly face an uphill battle in finding clinicians properly trained to treat them because most dentists lack the proper training and exposure with respect to the health and psychosocial needs of this population.
According to one study, more than 50 percent of dental and medical school deans have stated that their graduates are not competent to treat patients with I/DD; as a result, people with I/DD are more likely to have poor oral hygiene, periodontal disease, and untreated dental caries than are members of the general population.
People with I/DD have been more likely to not have had their teeth cleaned in the past five years, or never to have had their teeth cleaned, than those who are not disabled.
Due to the lack of proper skills among dentists, dental care is often more difficult to find than any other type of service for people with I/DD.
Last year, NCD successfully worked with the American Dental Association to revise its Code of Professional Conduct to state that “dentists shall not refuse to accept patients into their practice or deny dental service to patients because of the patient’s disability.” This code revision was adopted by many states as state law of professional conduct.
The following is written by Elluz Peraza, the community specialist and radio show host and producer for CV Global. She provides care for her 100-year-old mother, who lives with her. Peraza is a former actress and was Miss Venezuela1976.
According to AARP, more than 40 million people in the United States are providing care for an older or aging loved one – and 7 million of us are Latinos. That doesn’t come as any surprise to members of our community. It’s simply what we do for family. For many, caregiving starts with simple errands and to-do items, like scheduling a doctor’s appointment or helping out with grocery shopping and, then, expands to more responsibilities over time.
It’s a beautiful thing to do what we can for the people we love, but there are also moments when we can feel worn out or stretched too thin.
When you look at the numbers, it’s clear how hard we’re working. Nearly 7-in-10 Latino caregivers work outside the home. 1-in-3 provide more than 40 hours of care to loved ones each week. You do the math. It doesn’t add up to much time for the “life” side of a caregiver’s work-life balance.
That’s why AARP and the Ad Council started a Caregiver Assistance campaign to offer information and free online resources for caregivers. On AARP’s Family Caregiving site, there are wellness tips, planning resources, financial guidance and Care Guides tailored to specific topics and challenges, such as caring for a loved one with dementia. It also includes self-care tips and advice for caregivers.
Throughout my own caregiving experience, here are some helpful tips I’ve learned along the way:
1. Care for yourself.
You cannot care for your loved ones unless you care for yourself. It’s important, not only to your mental well-being, but your physical well-being, too. Caregivers have a higher-than-normal rate of getting sick, and are oftentimes so depleted that they can’t care for either their loved one or themselves. Look after your own health by eating well-balanced meals, exercising, getting enough sleep and taking time off.
2. Stay organized with handy tools.
You’re probably already an expert at organizing documents and medical cards, insurance papers and everything else. Make your life a little easier by leaning on free resources that can help you keep everything together! There are a ton available for your needs on AARP’s Family Caregiving site.
3. Remember to laugh.
Caring for someone with significant impairments or illness can be difficult emotionally, but laughter and lightness can exist there, too. Joke with your loved one – he/she is still the same person inside – and try to be amused by the little things.
4. Make future plans.
When a loved one you’ve been caring for passes away, it can come as a shock. You might feel like your purpose is gone and this can exacerbate the grieving process. Planning for the future will help relieve that shock for you, even if the plans aren’t concrete. Dream about the exciting roads ahead, and keep in mind all the incredible ways you’ve learned and grown through caregiving.
5. Accept help.
Whether it’s from other family members or outside sources, help is critical to caregivers. Start with the free resources that AARP can offer you at aarp.org/cuidar (Spanish) and aarp.org/caregiving (English) or feel free to call the hotline: 1-888-971-2013 (Spanish) or 1-877-333-5885 (English).
I was about 31 when I was first diagnosed with major depression. I was married, had two beautiful kids ages 7 and 3, and owned a thriving business. Despite having plenty to live for, my usual happy mood had plummeted into despair. I’d lie awake at night ruminating about every minor thing I had ever said or done wrong – or imperfectly. During the day, I had no motivation to do anything. The most simple everyday tasks suddenly required extraordinary effort. My life felt utterly worthless, despite all evidence to the contrary, and I was engulfed in sorrow and hopelessness.
As days turned into weeks, I continued to spiral on a downward path. I became increasingly focused on death. I wasn’t suicidal, per se – though thoughts of the least painful methods of ending my suffering certainly swirled around in my mind. But I wanted nothing more than to fall asleep and never wake again.
Finally, unable to endure the emptiness any longer and terrified by my thoughts, I sought help. I was immediately started on an antidepressant and, within a few short weeks, the darkness lifted. I was my usual happy, energetic self once again.
But this was only the beginning of what would become a lifelong battle with depression. Over the past couple of decades, I’ve gone through far too many bouts of depression to count. Some have been mild and short-lived having little impact on my functioning despite the bleak and gloomy outlook looming over me. Other episodes have been major and affected all aspects of my life.
Most recently, I experienced my first dysthymic episode – a depression that lasted two years, cycling between mild and severe. I had become resistant to my long-trusted friend, Wellbutrin, and none of the many other medications I tried gave me any relief. It was when I finally found apsychopharmacologist who knew just the right cocktail (combination of medications) for me that my depression finally went back into remission.
People with depression often suffer from various forms. In addition to being diagnosed with major depressive disorder and dysthymia, I’ve also been diagnosed with seasonal affective disorder (SAD) and bipolar II (hypomania, rather than mania) with the depression component being the more severe problem for me.
photo credit: CDC
Women are particularly at risk for depression
Depression does affect both women and men. But, women are twice as likely to experience major depression according to Harvard Medical School. Women also experience higher rates of dysthymia, seasonal affective disorder (SAD), and the depressive side of bipolar disorder.
Depression, unlike the normal sadness everyone experiences from time to time, is a soul-sucking darkness that for many is debilitating. It causes feelings of hopelessness, helplessness, and worthlessness, and can affect every aspect of life from work and school to parenting, friendships, and the very basics of living.
For most women who’ve been diagnosed with depression in the past, when it begins to set in, the feeling is unmistakable. But for those who suffer from milder forms of depression and sometimes even those suffering from a first major depressive episode, they don’t immediately connect all the dots. So, some people can experience depression not realizing they’re suffering from a treatable illness.
Signs of depression
The symptoms of depression can range from mild to severe. Not everyone experiences every symptom. But several symptoms must be present for at least two weeks to receive a diagnosis of depression. The exact criteria for specific types of depression vary slightly. But the following are all indicators.
· Feeling depressed (sad, empty, or hopeless) nearly every day for at least a couple weeks
· Unusual irritability or difficulty controlling anger
· Ongoing trouble sleeping or sleeping more than usual
· An increase or decrease in appetite or significant unexplained weight loss or gain
· Loss of interest or pleasure in all or most activities
· Difficulty concentrating or making decisions
· Feelings of fatigue or loss of energy
· Excessive or inappropriate feelings of guilt or worthlessness
· Visible psychomotor slowing down or agitation
· Recurrent thoughts of death or suicide, with or without a plan, or attempted suicide
photo credit: CDC
Types of depression
There are quite a few classifications, or types, of depression. The following are a few of the more common.
In a given year, major depressive disorder affects nearly 7% of U.S. population, according to the National Institutes of Mental Health (NIMH). During a major depression, almost all aspects of a person’s life are affected. It can be difficult for someone with major depression to find the motivation to do anything including such necessities as taking a shower. As a result of the impairment, both work and personal life suffer. In addition to the symptoms in the section above, 20% of people with major depression will also experience psychosis. This means they’ll experience hallucinations and delusions.
Dysthymia is diagnosed when a person has experienced depression for most of each day and on most days for at least two years. For many, it’s a lower level but enduring depression. But people with major depression who are treatment resistant can meet the diagnosis of dysthymia as well. So those with dysthymia can range from mild to severe impairment. Women, according to HealthFundingResearch.org, are three times more likely than men to suffer from dysthymia.
Those with seasonal affective disorder (SAD) become depressed only or primarily during a particular season. For most with SAD, it’s the fall and winter months with their shorter days and reduced sunshine. But some people experience SAD during the summer months instead. The onset of SAD is typically around the age of 20 and affects 10 million Americans each year.
Bipolar disorder affects 2.6% of American adults according to the NIMH. This treatable, but lifelong disease typically develops in women in their mid to upper 20s. For men, onset is usually in the teens to the early 20s. Bipolar is signified by its bouts of both mania (or hypomania) and its opposite extreme, depression. Though an individual with bipolar will experience both sides of the spectrum, in women, depression is often the most problematic while for men it’s the mania. Those with bipolar often experience psychosis during bouts of mania and sometimes with depression.
Postpartum depression is one of the forms of depression exclusive to women. According to the NIMH, 10-15% of women will develop it. Postpartum depression shouldn’t be confused with the “baby blues,” which is milder, short-lived, and related to the worry and fatigue of parenting a new baby. Instead, postpartum depression results from hormonal changes. During pregnancy, a woman’s hormone levels increase. But then immediately following childbirth, the hormone levels rapidly drop to normal levels. This ultimately results in depression in some women. Like other forms of depression, it can be mildly to severely debilitating.
photo credit: CDC
Causes
The exact cause of depression is unknown. But several factors likely contribute to the condition. According to the Mayo Clinic, those with depression have physical changes in their brains. These changes in the brain may eventually help researchers determine the exact cause of depression.
Depression is also known to be genetic because of the higher incidence of depression in those with blood relatives who suffer from the condition.
Brain chemicals called neurotransmitters play a role in depression. The Mayo Clinic explains that the way the neurotransmitters function and how they affect the neurocircuits involved in mood stability plays a significant role both in depression and its treatment.
Hormonal changes can also play a role in depression, particularly for women. During pregnancy and for several months following pregnancy women are especially vulnerable. Menstruation cycles and menopause can also trigger depression.
Treatment
In some cases, depression results from an underlying medical condition such as thyroid problems or low vitamin B levels. For this reason, it’s essential to visit your primary care physician for blood work to rule out other causes. If the cause of depression is the result of an underlying medical condition, treatment for that condition is likely all that’s needed to cure the depression.
If medical causes have been ruled out, then it’s best to consult with a psychiatrist. Although primary care physicians can treat depression, psychiatrists have specialized training in diagnosing the various forms of depression and experience in treating them. Psychiatrists often know which medications will work best for a particular patient based on a variety of factors. In fact, depending on the type of depression and the specific set of symptoms, some people with depression require a combination of anti-depressants, anti-anxiety medications, and mood stabilizers. Psychiatrists know how to tailor treatment to each individual for best results.
For those who are treatment resistant, look for a psychiatrist with the special ‘psychopharmacologist’ designation. Psychopharmacologists have gone through additional specialized training in how drugs affect the mind and behavior.
In addition to medication, many psychiatrists recommend cognitive therapy with a psychologist or behavioral therapist in conjunction.This can be helpful both in coping with the effects of depression as well as dealing with any underlying trauma or events fueling the depression.
Finally, for those with SAD, sitting under a light therapy box is often recommended and has been found to be helpful. You can order one online and, depending on your doctor’s recommendations, you can sit under it for 20-40 minutes each day.